Foto
Video
Audio
Vektoren
Benutzername:
Passwort:
Passwort vergessen
Kostenlose Registrierung
Foto
Video
Audio
Vektoren
Mein Profil
Warenkorb
(
0
)
Leuchtkästen
( 0 )
schnelle Hilfe
en
de
en
us
eu
fr
es
mx
Es ist kein Fehler aufgetreten
Hinweis!
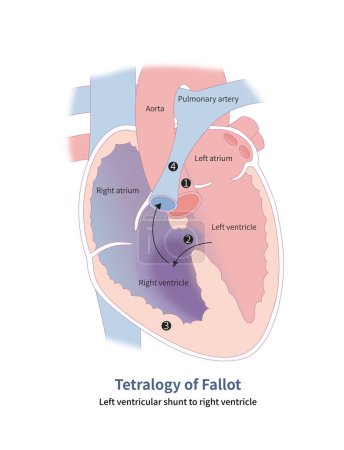
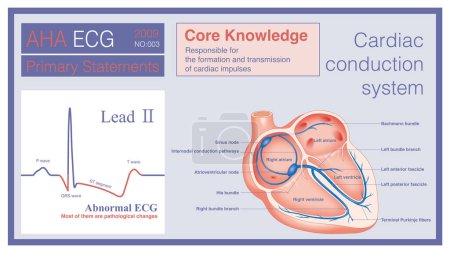
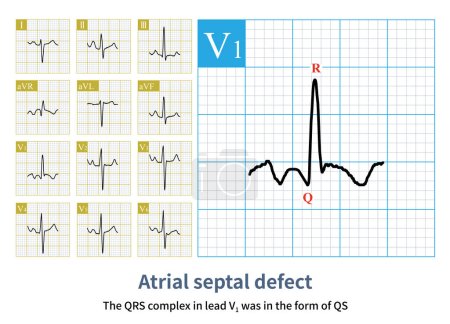
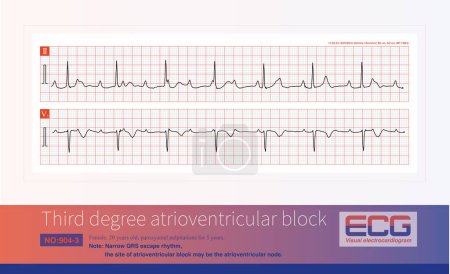
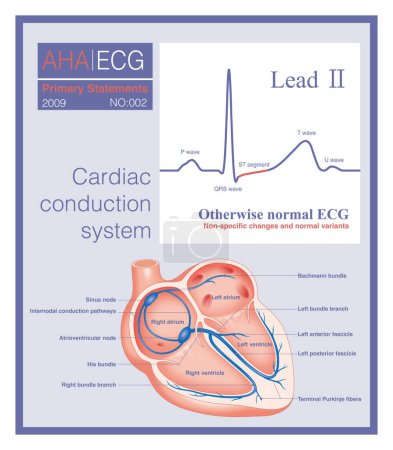
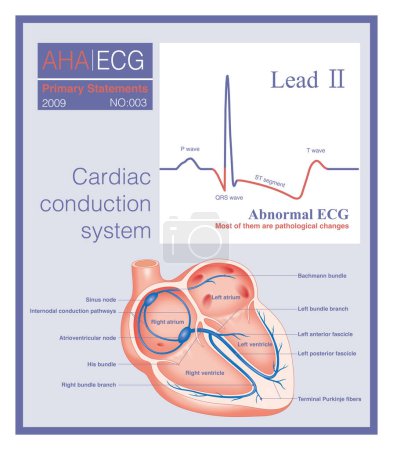
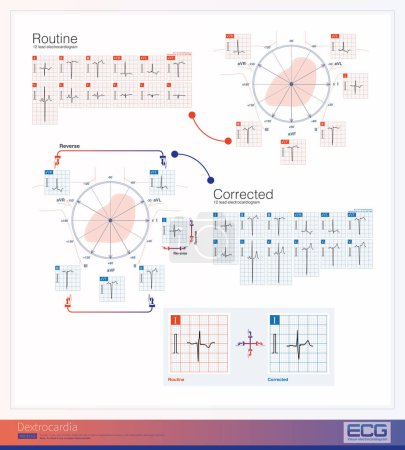
103 Bilder zum Thema "st segment" bei ClipDealer
alle Filter zurücksetzen
Medien sortieren nach
Datum
Bewertungen
Aufrufen
Relevanz
Download
aufsteigend
absteigend
Gehe zu Seite:
« Vorherige
1
2
Nächste »
Nächste Seite »
« Vorherige
1
2
Nächste »